From Sun Fear to Sun Debt
Over recent decades, public health messaging, workplace patterns, and beauty culture have converged to create a quiet epidemic of sun avoidance. Melanoma awareness campaigns, particularly in high-incidence regions such as Australia, North America, and Norther Europe, have justifiably emphasized the carcinogenic potential of ultraviolet radiation and strongly promoted sun-protective behaviours including sunscreen use, shade seeking, and clothing barriers. At the same time rapid urbanization, indoor and screen-based work, and cosmetic anti-aging have normalised a lifestyle in which many individuals spend most of their days under artificial light, encountering natural sunlight only in brief, incidental doses.
Against this backdrop of “sun phobia,” an emerging body of epidemiological evidence suggests that very low habitual sun exposure may carry its own, substantial health cost. Large Scandinavian cohorts, including Swedish women with prospectively recorded sun-exposure habits, show that individuals who consistently avoid the sun experience approximately double the all-cause mortality of those with the highest sun-exposure habits, largely driven by cardiovascular and other non-cancer causes of death. Complementary modelling work estimates that insufficient sun exposure may contribute to hundreds of thousands of deaths annually in Europe and the United states, and is associated with higher burdens of cardiometabolic disease, certain internal cancers, autoimmune conditions and neurodegenerative disorders. Together, these data begin to reframe sunlight from a purely dermatologic risk to a systemic health determinant, where both extremes, chronic overexposure and chronic avoidance may be hazardous for long-term survival.
The Swedish Wake-Up Call: When Sun Avoidance Rivals Smoking
The Melanoma in Southern Sweden (MISS) cohort has become a pivotal natural experiment for understanding the long-term consequences of habitual sun avoidance on survival. In this prospective study, 29,158 women aged 25-64 years were recruited between 1990 and 1992 and followed for approximately two decades, with detailed baseline data on sun-exposure habits (such as sunbathing in summer and winter, use of tanning beds, and holidaying in sunny climates) and a broad range of potential cofounders including age, smoking, socioeconomic status, and comorbidities. Using flexible parametric survival models, investigators consistently observed an inverse, dose-dependent relationship between sun exposure and all-cause mortality: women who reported avoiding active sun exposure had roughly double the mortality rate of those in the highest sun exposure category, corresponding to an estimated population, attributable risk of about 3% for death associated with sun-avoidant behaviour in this cohort [1].
Subsequent competing risk analyses of the same MISS cohort extended these findings by disentangling causes of death and quantifying effects on life expectancy. Women with more active sun-exposure habits had substantially lower cardiovascular and non-cancer/non-cardiovascular mortality but, as a consequence of living longer, a higher relative proportion of deaths from cancer, including melanoma, compared with strict sun avoiders. Strikingly, when then analysis was restricted to nonsmokers, those who avoided sun exposure had a life expectancy comparable to smokers in the highest sun-exposure group, leading the authors to conclude that avoidance of sun exposure appears to be a risk factor for death of a similar magnitude as smoking in this population. This “Swedish wake-up call” does not negate the carcinogenic potential of ultraviolet radiation, but it reframes chronic sun avoidance, from seemingly harmless preventive behaviour to a potential major determinant of premature mortality that must be weighed alongside smoking, physical inactivity, and other established lifestyle risks [1,2,3,4,5].
Beyond One Cohort: What the Broader Sun Mortality Literature Shows
Beyond the MISS cohort, several Scandinavian and European studies support a broader pattern in which higher natural sun exposure is associated with reduced mortality from major chronic diseases. In a large Swedish cohort of 38,472 women, those who reported sunbathing vacations more than once a year over three decades had significantly lower all-cause and cardiovascular mortality than women who rarely travelled for sun, even though their overall cancer incidence and the proportion of deaths due to cancer were higher. Compilations of these and related cohorts, summarized in European public-health reviews, reinforce the notion that regular, non-artificial UV exposure appears linked to lower risks of cardiovascular disease, hypertension, metabolic syndrome, and several internal cancers, while artificial tanning (solarium use) consistently shows increased all-cause and cancer mortality [6,7,8].
Recent systematic reviews of sunlight exposure and mortality paint a more nuanced picture that balances benefits and harms. A 2025 NIHR-commissioned review identified cohort and ecological studies in which higher sunlight or UV indices were associated with lower all-cause and cardiovascular mortality, but also studies where markers of chronic actinic skin damage correlated with increased cardiovascular death, highlighting how cumulative overexposure may signal higher risk. Narrative and quantitative syntheses now emphasize that the mortality impact of sunlight depends on dose, pattern (regular non-burning vs intermittent intense exposure), latitude, ambient UV, and host phenotype, so that the same UV dose can be protective in high-latitude, vitamin D deficient populations yet harmful in fair-skinned individuals with high lifetime actinic damage. Collectively, this broader literature supports a U-shaped paradigm in which both insufficient and excessive sun exposure may increase mortality, and where carefully calibrated, context-specific sun habits offer the greatest potential for health span benefits [6,8,9,10].
Mechanistic Pathways: Why Sunlight Could Be Life-Preserving
The epidemiological association between low sun exposure and excess mortality is undergirded by a growing understanding of mechanistic pathways through which sunlight may exert life-preserving effects. The most established pathway involves vitamin D synthesis: ultraviolet B radiation (UVB, 290-315 nm) photochemically converts 7-dehydrocholesterol in the epidermis to previtamin D ~ 3~, which is isomerized and subsequently hydroxylated in the liver and kidney to 25-hydroxyvitamin D [25(OH)D] and 1,25-dihydroxyvitamin D, the active hormone. Large meta-analyses of prospective cohorts consistently demonstrate that individuals with serum 25(OH)D in the lowest quantile (0-9ng/mL) have approximately double the age-adjusted all-cause mortality hazard ratio compared with those in the highest quantile (>30ng/mL), with a steep dose-response gradient below 30ng/mL and apparent plateauing above 40-50ng/mL. Corresponding meta-analyses of randomized controlled trials indicate that vitamin D~3~supplementation (but not vitamin D~2~) modestly reduces overall mortality, particularly among older adults, with pooled relative risks of approximately 0.93-0.97 for all-cause mortality, and stronger inverse association observed with cardiovascular and cancer-specific death in observational studies [11,12,13,14].
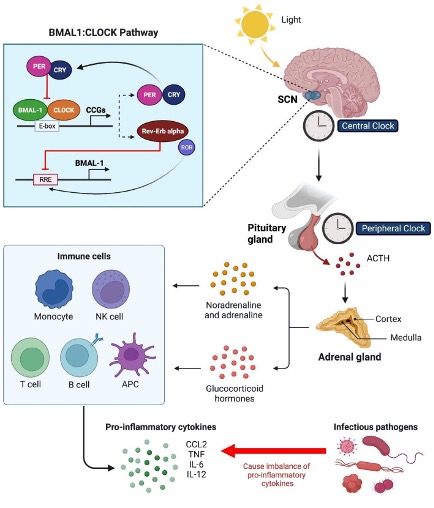
Beyond vitamin d, sunlight induces a suite of molecular and systemic effects that are independent of endocrine pathways. Ultraviolet a (UVA, 320-400nm) irradiation of human skin mobilizes performed nitric oxide (NO) from cutaneous stores, predominantly nitrate and nitrite pools into the systemic circulation, where NO exerts potent vasorelaxant activity through smooth muscle guanylate cyclase signalling. In controlled human studies, two standard erythemal doses of UVA acutely lower systolic and diastolic blood pressure, with concomitant decreases in circulating nitrate and rises in nitrite, and these hemodynamic effects occur independently of nitric oxide synthase activity and dietary nitrate availability, confirming mobilization from dermal and epidermal storage. Epidemiologically, incident solar UV exposure correlates inversely with blood pressure in large haemodialysis cohorts and seasonally with cardiovascular mortality, and experimental work demonstrates that low-dose daylight exposure (1 standard erythemal dose of UK sunlight) liberates NO with negligible DNA damage or cell death, suggesting a favourable benefit-harm window for moderate sun habits. Additional vitamin D independent mechanisms include circadian entrainment with innate and adaptive immune responses peaking and troughing according to local sunrise time, modulating susceptibility to respiratory and other infections and potential direct immunomodulatory effects on leukocyte trafficking, cytokine production, and pathogen clearance that are mediated by photoperiod, full-spectrum light, and time of day exposure patterns. Collectively, these pathways suggest that sunlight acts as a complex multimodal environmental input with pleiotropic systemic benefits that extend well beyond skeletal health, and that attempts to replicate sun exposure through oral supplementation capture only a fraction of its metabolic and cardiovascular advantages [6,15,16,17,18,19,20,21,22,23].
The Dark Side of Darkness: Health Cost of Chronic Sun Avoidance
While sun avoidance has become a cornerstone of melanoma prevention, observational and laboratory evidence now documents a suite of adverse consequences from chronic deficiency of natural ultraviolet exposure. Large epidemiological cohorts consistently demonstrate associations between very low sun exposure, severe vitamin D deficiency, and heightened risk of cardiovascular disease, metabolic disorders, autoimmune pathology, and increased all-cause mortality. A prospective U.S. cohort linking serum 25(OH)D levels below 15ng/mL with 1.62-fold higher cardiovascular even risk, rising to 2.13-fold among hypertensive individuals, exemplifies how severe deficiency potentiates cardiometabolic vulnerability through mechanisms including endothelial dysfunction, renin-angiotensin activation, vascular smooth muscle proliferation, and secondary hyperparathyroidism. Parallel data show that vitamin D deficiency co-occurring with metabolic syndrome further amplifies cardiovascular mortality (hazard ratio 1.77,95% CI 1.22-2.58) and all-cause mortality (hazard ratio 1.62, 95% CI 1.26-2.09), with the metabolic phenotype itself more prevalent in vitamin D-deficient groups, underscoring bidirectional links among sun debt, insulin resistance, dyslipidemia, and hypertension [6,24,25,26,27,28,29,30,31].
Clinical data from critically ill populations further illuminate how prolonged “sun debt” amplifies vulnerability in acute illness. Vitamin D deficiency (typically defined as <20-25 ng/mL) is detected 77-82% of intensive care unit (ICU) admissions, and sever deficiency (<12ng/mL) independently predicts doubled mortality risk even after adjustment for severity scores, with post-hoc analyses of ICU trials showing that patients with 25(OH)D £12ng/mL experience 32% 28 day mortality compared with 13% among those with higher levels. Mechanistic plausibility for these associations arises from vitamin D’s role in innate immunity including cathelicidin induction, T-cell regulation, and cytokine modulation and from its cardiovascular effects on vascular tone, cardiac remodelling, and thrombosis, all of which become critical in sepsis, acute respiratory distress syndrome, and multi-organ failure contexts where sunlight-deprived, chronically deficient individuals enter with depleted reserves. Taken together, these data suggest that chronic sun avoidance not only elevates baseline cardiometabolic and immune risk but may leave individuals physiologically ill-equipped to mount resilient responses to acute stressors translating “sun debt” into measurable excess mortality across the continuum from ambulatory to critical illness [6,32,33,34,35].
Skin Cancer, Melanoma, and The Dose-Response Paradox
The relationship between sunlight, skin cancer, and survival is characterized by a dose-response paradox in which the same exposure that clearly increases skin cancer risk may, in aggregate, be associated with lower overall mortality. Natural solar ultraviolet radiation (UVR) is well-established causal factor for keratinocyte cancer, basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) with occupational and high cumulative sun exposure consistently linked to higher incidence in fair-skinned populations. Intermittent, intense UV exposure and sunburns, particularly in childhood and adolescence are major determinants of cutaneous melanoma, with meta-analyses showing around 60% higher melanoma risk with recreational/intermittent sun exposure and an even stronger effect of histories of severe sunburn [36,37,38,39,40].
Yet, when mortality, not incidence is examined in longe-term cohorts, a different pattern emerges. In Swedish women followed for nearly 15 years, higher solar UV exposure, including more frequent sunbathing vacations and adolescent sunburns, was associated with reduced all-cause and cancer mortality. Competing-risk analyses of the melanoma in southern Sweden (MISS) cohort similarly showed that women with active sun-exposure habits had substantially lower cardiovascular and non-cancer/ non-cardiovascular mortality, resulting in longer life expectancy than sun avoiders. Because sun-seeking women lived longer, a greater proportion of their deaths were due to cancer including skin cancers creating the paradox of higher cancer incidence a higher share of cancer deaths in a group that nonetheless experienced fewer deaths overall and longer survival [7,41].
This dose-response paradox underscores the distinction between cause-specific risk and total mortality in longevity medicine. Sun exposure clearly increases the absolute risk of keratinocyte cancers and contributes to melanoma risk, particularly with fair phenotypes, intermittent intense exposures, and artificial UV sources; at the same time, moderate regular natural sun exposure appears to reduce fatal cardiovascular events and other non-cancer causes through vitamin D-dependent and -independent mechanisms. In countries with low ambient UV, very restrictive sun-avoidance advice may therefore shift the balance toward fewer skin cancers but more deaths overall, while carefully calibrated sun habits that prevent burning but avoid chronic deprivation may allow individuals to benefit from cardiometabolic and systemic effects of sunlight, even if this entails a modest increase in largely treatable skin cancer incidence [36,40,41,42,43,44].
Phenotype, Latitude, and Inequity: Who Pays the Highest Price for Sun Avoidance
Human adaptation to sunlight is not uniform, and the health costs of chronic sun avoidance fall unevenly across phenotypes and latitudes. In low-UV environments such as Sweden, a nested case-control analysis within the MISS cohort showed that women with fair, UV-sensitive phenotypes had significantly lower all-cause mortality than non-fair women when both groups had low-to-moderate sun exposure, with an approximately 8% lower mortality rate despite a higher risk of dying from skin cancer. These findings support the idea that fair skin, which permits more efficient cutaneous vitamin D synthesis at high latitudes, may confer a survival advantage in a low-UV milieu, but at the cost increased skin cancer susceptibility, suggesting historical selection for lighter pigmentation as an adaptation to limited UVB [[42,45].
By contrast, dark-skinned dark‑ skinned individuals living at high latitudes or in low‑UV settings are disproportionately prone to vitamin D deficiency and its downstream risks. Population data from the United States show that severe deficiency (25(OH)D <10 ng/mL) is found in about 17% of non‑Hispanic Black adults versus 1% of non‑Hispanic whites, and overall deficiency (<20 ng/mL) affects roughly three‑quarters of Black adults compared with one‑fifth of whites, a disparity that is magnified with increasing distance from the equator and time since migration. Similar patterns are reported among African, Middle Eastern, and South Asian immigrants to Northern Europe, where 25(OH)D <50 nmol/L is the norm rather than the exception, and is associated with higher burdens of cardiometabolic disease, pregnancy complications, and possibly cancer. These latitude–phenotype mismatches mean that applying the same stringent sun‑avoidance recommendations to all skin types can over‑protect fair‑skinned, low‑latitude populations from relatively treatable keratinocyte cancers while under‑recognizing the excess mortality risk from chronic vitamin D deficiency and “sunshine deficiency” in darker‑skinned, high‑latitude communities [6,46,47,48,49].
From a public-health perspective, this heterogeneity argues strongly against one-size-fits-all “avoid the sun” messaging. Reviews on insufficient sun exposure now estimate that low sunlight may contribute to hundreds of thousands of deaths per year in North America and Europe through increased rates of cardiovascular disease, metabolic syndrome, certain cancers, multiple sclerosis, and other chronic conditions, and explicitly call for phenotype and latitude- specific guidance that balances skin-cancer prevention with systemic health. For fair-skinned individuals in high-UV environments strict burn avoidance, protective clothing, and intermittent shade remain crucial, but for dark-skinned individuals living at higher latitudes, policies should prioritize adequate safe sun exposure, vitamin D monitoring, and supplementation where necessary, rather than reflexive UV avoidance. Framing sun exposure as an equity issue where those with the least physiological capacity to synthesize vitamin D are often advised to hide from the sun under blanket guidelines, highlights the need for nuanced, context-sensitive “sun hygiene” strategies that explicitly account for phenotype, latitude, culture, and baseline disease risk [6,42,45,46,50].
Sunlight vs Pill: Can Vitamin D Supplements Replace the Sun?
Randomized trials and observational data suggest that vitamin D supplements can modestly reduce mortality, but they do not appear to reproduce the full survival advantage seen in people with natural higher sun exposure. Ealy meta-analyses of randomized controlled trials involving more than 57,000 participants reported that daily cholecalciferol in typical doses (300-2m000 IU) reduced all-cause mortality by about 7% (summary relative risk 0.93; 95% CI 0.87-0.99), with signals for greater benefit in longer-duration trials and when baseline 25(OH)D levels were low. More recent, larger meta-analyses including 50 trials and over 74,000 participants have refined this picture: vitamin D supplementation has little nor no effect on all-cause mortality overall (risk ratio 0.98; 95% CI 0.95-1.02) but does reduce cancer mortality by roughly 15%, particularly with vitamin D3 and longer follow-up. Individual-participant-data analyses from European cohorts, however, show that low serum 25(OH)D (<30-40nmol/L) is associated with 33-67% higher all-cause mortality compared with levels 75-100nmol/L, and high sun-exposure cohorts exhibit larger survival gaps between sun avoiders and sun seekers than supplementation trials alone can explain. This divergence suggests that pharmacologic correction of vitamin D captures only part of the mortality benefit associated with living a sun-exposed life [11,12,51,52,53,54].
One likely explanation is that sunlight is a complex exposure comprising spectral composition, intensity, timing, and body-surface distribution, which collectively engage multiple psychological systems beyond vitamin D synthesis. Full- spectrum daylight entrains circadian clocks in the suprachiasmatic nucleus and peripheral tissues, modulating sleep architecture, autonomic balance, and immune timing in ways not replicated by oral vitamin D alone. UVA and visible wavelengths mobilize nitric oxide from cutaneous stores, lower blood pressure, and may improve vascular function and cardiometabolic risk independent of 25(OH)D concentrations, while thermal and behavioural correlates of outdoor light (movement, social contact, environmental enrichment) further differentiate natural sun exposure from pill-based replacement. Recent integrative reviews therefore argue that moderate sun exposure should be viewed as a co-therapy rather than a competitor to supplementation: a low-cost, multifaceted environmental input that corrects vitamin D insufficiency, supports cardiovascular and immune health, and may enhance survival beyond what “sun in a capsule” can deliver, provided that exposure is carefully titrated to avoid burns and excessive cumulative UV damage [16,20,22,55,56,57,58,59,60].
Towards a “ Safe Sun” Prescription: Translating Evidence into Practice
Translating the emerging sun, mortality evidence into practice requires a move from binary “good vs bad” ultraviolet messaging toward a balanced “safe fun” prescription that can be individualized in the same way as blood pressure or lipid targets. Contemporary public health analyses argue that non-burning UV exposure is a health benefit and, in moderation should be recommended as such, given accumulating data that insufficient sun exposure is associated with increased risk of cardiovascular disease, metabolic syndrome, some internal cancers, and higher all‑cause mortality. A practical framework centers on short, regular, non‑burning exposures tailored to skin type, latitude, season, and personal cancer risk: for light skin at mid‑latitudes, this may mean only a few minutes of midday sun with 25–35% body surface exposed; for darker skin or higher latitudes, substantially longer exposures or greater surface area may be needed to achieve similar vitamin D effective doses without erythema. Position statements from expert groups therefore increasingly emphasize exposing more skin for less time, using shade, clothing, and sunscreens to avoid sunburn and protect high‑risk anatomic sites (face, neck, ears, shoulders), rather than blanket avoidance of outdoor sun when the UV index is modest [6,10,44,61,62,63,64].
Operationalizing this “safe sun” concept in aging‑well and metabolic clinics invites a more systematic approach to sun as a vital sign. Routine preventive assessments could include a brief sun‑exposure history (time outdoors, work pattern, sunscreen and clothing habits, holidays, tanning‑bed use), objective or estimated vitamin D status, and phenotypic skin‑cancer risk (Fitzpatrick skin type, nevi, personal or family history of skin cancer), alongside cardiometabolic parameters. From these inputs, decision‑support tools and AI‑enabled models could generate personalized sun‑exposure targets, specifying safe time windows by season and UV index, approximate minutes to first erythema for that skin type at the local latitude, suggested frequency and body‑surface area, and when to prioritize supplementation or photoprotection instead. At a population level, integrated electronic records could flag individuals at highest risk from “sun debt” (dark‑skinned at high latitude, institutionalized older adults, those with chronic disease and low 25(OH)D) for proactive counselling and monitoring, while also identifying fair‑skinned individuals with heavy lifetime UV burden who require stringent anti‑burn strategies. In this model, sun exposure becomes a quantifiable, titratable environmental therapy, co-managed with smoking cessation, physical activity, nutrition and sleep, rather than an unmeasured, all-or-nothing hazard, bringing preventive care closer to a genuinely personalized, longevity-oriented standard [6,10,44,56,61,62,65,66].
“Sun Avoidance as Deadly as Smoking” Without Fearmongering
The phrase “sun avoidance as deadly as smoking” derives its theorical force from robust but context-specific observational data and therefore demands careful framing in public communication. Analyses from the Melanoma in Southern Sweden cohort found that women who consistently avoided sun exposure had approximately double the all‑cause mortality of those with the highest sun‑exposure habits, and that nonsmokers who avoided the sun had a life expectancy similar to smokers in the highest exposure group. However, these findings come from a single, predominantly fair‑skinned Scandinavian cohort and are subject to the usual limitations of observational design, residual confounding, unmeasured health behaviours, and restricted generalizability, so any “as deadly as smoking” slogan should be explicitly anchored to this context rather than presented as a universal, causal equivalence [1].
Used responsibly, strong framing can serve as a heuristic to open nuanced conversations about “safe sun,” not as an invitation to unprotected exposure or indoor tanning. Communication strategies should pair the headline with clear caveats that chronic sun avoidance and chronic burning are both harmful; that recommendations must differ by skin type, latitude, and cancer risk; and that artificial UV from sunbeds is consistently classified as carcinogenic, associated with markedly higher melanoma, basal cell, and squamous cell carcinoma risks and increased mortality. In social media and patient education, the narrative arc can move from the surprising Swedish data to practical guidance: brief, regular, non‑burning natural sun exposure plus strong discouragement of tanning‑bed use, emphasizing that the goal is not “more sun at any cost” but calibrated exposure that captures systemic benefits while minimizing skin‑cancer risk [67,68,69,70].
From UV Enemy to Essential Exposure in Longevity Medicine
A growing body of evidence suggests that sunlight should no longer be viewed solely as an environmental carcinogen to be minimized, but as a modifiable exposure with a bidirectional risk profile in longevity medicine. Cohorts such as the Melanoma in Southern Sweden (MISS) study demonstrate that women with active sun-exposure habits have lower cardiovascular and non-cancer mortality and liver longer overall, even though their relative proportion of cancer death is higher because they survive competing causes of death. At the same time, public health directives and narrative reviews now argue that insufficient sun exposure has become a real public health problem, potentially contributing to hundreds to thousands of deaths annually in Europe and the United States, while excessive exposure and sunburn remain clearly linked to keratinocyte cancers and melanoma. Taken together, these data support reframing sunlight as a continuum in which both extremes, chronic avoidance and chronic burning are hazardous, and in which moderate, non-burning, individualized sun habits may play an important role in supporting longer, healthier lives.
This reframing has direct implications for standards of care in aging and metabolic wellness. Rather than promoting blanker UV avoidance, emerging reviews and expert statements call for guidance that integrates skin phenotype, latitude, season, and cardiometabolic risk, with practical recommendations such as brief (5-30 minute) non-burning exposures adjusted to UV index and skin type, combined with targeted protection at higher doses or for high-risk individuals. Future preventive frameworks should test “sun hygiene” alongside smoking cessation, cardiorespiratory fitness, nutrition, and sleep as a core pillar of health span extension, including routine assessment of sun-exposure habits, vitamin D status, and skin-cancer risk, and the use of decision support and AI-enabled tools to personalize safe-sun prescriptions across diverse phenotypes latitudes. By embedding sunlight within a nuanced, data-driven model of exposure rather than an absolute threat, longevity medicine can move toward a more complete, system level approach to environmental inputs that shape cardiometabolic resilience, immune function, and overall survival.
Reference
- Lindqvist PG, Epstein E, Landin-Olsson M, Ingvar C, Nielsen K, Stenbeck M, et al. Avoidance of sun exposure is a risk factor for all-cause mortality: results from the Melanoma in Southern Sweden cohort. Journal of Internal Medicine. 2014 Apr 23;276(1):77–86.
- Jablonski NG. Is there a golden mean for sun exposure? Journal of Internal Medicine. 2014 Apr 4;276(1):71–3.
- Lindqvist PG, Olsson H. Are low sun exposure habits a genuine strong risk factor for all‐cause mortality or the result of bias? Journal of Internal Medicine. 2017 Mar 24;281(6):620–1.
- Lindqvist PG, Landin-Olsson M, Olsson H. Low sun exposure habits is associated with a dose-dependent increased risk of hypertension: a report from the large MISS cohort. Photochemical & Photobiological Sciences. 2021 Feb;20(2):285–92.
- Lindqvist PG, Epstein E, Nielsen K, Landin-Olsson M, Ingvar C, Olsson H. Avoidance of sun exposure as a risk factor for major causes of death: a competing risk analysis of the Melanoma in Southern Sweden cohort. Journal of Internal Medicine. 2016 Mar 16;280(4):375–87.
- Alfredsson L, Armstrong BK, Butterfield DA, Chowdhury R, de Gruijl FR, Feelisch M, et al. Insufficient Sun Exposure Has Become a Real Public Health Problem. International Journal of Environmental Research and Public Health [Internet]. 2020 Jul 1;17(14). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7400257/
- Yang L, Lof M, Veierød MB, Sandin S, Adami HO, Weiderpass E. Ultraviolet Exposure and Mortality among Women in Sweden. Cancer Epidemiology Biomarkers & Prevention. 2011 Feb 4;20(4):683–90.
- Monserrat-García MT, Ortíz-Prieto A, Martín-Carrasco P, Conejo-Mir-Sánchez J. RF- Insufficient Exposure to Sunlight and Global Mortality: Should We Advise Against or Recommend Sun Exposure? Actas Dermo-Sifiliográficas (English Edition). 2017 Apr;108(3):257–8.
- Parkhouse T, Spiga F, Rhodes LE, Dawson S, Webster KE, Caldwell DM, et al. The effects of sunlight exposure on mortality: a systematic review of epidemiological studies. NIHR Open Research [Internet]. 2025 Nov 28 [cited 2026 Jan 6];5:51. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC12709114/
- Hoel D, de Gruijl F. Sun Exposure Public Health Directives. International Journal of Environmental Research and Public Health. 2018 Dec 10;15(12):2794.
- Garland CF, Kim JJ, Mohr SB, Gorham ED, Grant WB, Giovannucci EL, et al. Meta-analysis of All-Cause Mortality According to Serum 25-Hydroxyvitamin D. American Journal of Public Health. 2014 Aug;104(8):e43–50.
- Autier P. Vitamin D Supplementation and Total MortalityA Meta-analysis of Randomized Controlled Trials. Archives of Internal Medicine [Internet]. 2007 Sep 10;167(16):1730. Available from: https://jamanetwork.com/journals/jamainternalmedicine/article-abstract/413032
- Gaksch M, Jorde R, Grimnes G, Joakimsen R, Schirmer H, Wilsgaard T, et al. Vitamin D and mortality: Individual participant data meta-analysis of standardized 25-hydroxyvitamin D in 26916 individuals from a European consortium. PLoS ONE [Internet]. 2017 Feb 16 [cited 2020 May 14];12(2). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5312926/
- Chowdhury R, Kunutsor S, Vitezova A, Oliver-Williams C, Chowdhury S, Kiefte-de-Jong JC, et al. Vitamin D and risk of cause specific death: systematic review and meta-analysis of observational cohort and randomised intervention studies. BMJ [Internet]. 2014 Apr 1;348(apr01 2):g1903–3. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3972416/
- Cao M, He C, Gong M, Wu S, He J. The effects of vitamin D on all-cause mortality in different diseases: an evidence-map and umbrella review of 116 randomized controlled trials. Frontiers in Nutrition [Internet]. 2023 Jun 22;10. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10325578/
- Wang C, Lutes LK, Barnoud C, Scheiermann C. The circadian immune system. Science Immunology. 2022 Jun 3;7(72).
- Mo Z, Scheben A, Steinberg J, Siepel A, Martienssen R. Circadian immunity, sunrise time and the seasonality of respiratory infections. 2021 Mar 31 [cited 2025 Apr 25]; Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC8020986/
- Weller RB, Wang Y, He J, Maddux FW, Usvyat L, Zhang H, et al. Does Incident Solar Ultraviolet Radiation Lower Blood Pressure? Journal of the American Heart Association. 2020 Mar 3;9(5).
- Liu D, Fernandez BO, Hamilton A, Lang NN, Gallagher JMC, Newby DE, et al. UVA Irradiation of Human Skin Vasodilates Arterial Vasculature and Lowers Blood Pressure Independently of Nitric Oxide Synthase. Journal of Investigative Dermatology. 2014 Jul;134(7):1839–46.
- Hazell G, Khazova M, O’Mahoney P. Low-dose daylight exposure induces nitric oxide release and maintains cell viability in vitro. Scientific Reports [Internet]. 2023 Sep 28;13(1):16306. Available from: https://www.nature.com/articles/s41598-023-43653-2
- Huang H, Mehta A, Kalmanovich J, Anand A, Bejarano MC, Garg T, et al. Immunological and inflammatory effects of infectious diseases in circadian rhythm disruption and future therapeutic directions. Molecular Biology Reports. 2023 Jan 19;
- Quan Q, Yoon K, Lee JS, Kim EJ, Lee DH. Impact of ultraviolet radiation on cardiovascular and metabolic disorders: The role of nitric oxide and vitamin D. Photodermatology Photoimmunology & Photomedicine. 2023 Sep 20;39(6):573–81.
- Chertoff M, Marpegan L, Nicolás Pregi, Paladino N. Editorial: The Circadian Clock and immune system interplay in infectious diseases. Frontiers in Cellular and Infection Microbiology. 2022 Oct 25;12:1036633–3.
- Sizar O, Khare S, Goyal A, Bansal P, Givler A. Vitamin D Deficiency [Internet]. PubMed. Treasure Island (FL): StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532266/
- Liu L, Cui S, Volpe SL, May NS, Sukumar D, DiMaria-Ghalili RA, et al. Vitamin d deficiency and metabolic syndrome: The joint effect on cardiovascular and all-cause mortality in the United States adults. World Journal of Cardiology [Internet]. 2022 Jul 26 [cited 2022 Nov 14];14(7):411–26. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9350604/
- Mozos I, Marginean O. Links between Vitamin D Deficiency and Cardiovascular Diseases. BioMed Research International. 2015;2015:1–12.
- Wang H, Chen W, Li D, Yin X, Zhang X, Olsen N, et al. Vitamin D and Chronic Diseases. Aging and disease [Internet]. 2017;8(3):346. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5440113/
- Insufficient Sun Exposure is a Public Health Concern – GrassrootsHealth [Internet]. GrassrootsHealth. 2021 [cited 2026 Jan 6]. Available from: https://www.grassrootshealth.net/blog/insufficient-sun-exposure-public-health-concern/
- Giustina A, Bilezikian JP, Adler RA, Banfi G, Bikle DD, Binkley NC, et al. Consensus statement on vitamin D status assessment and supplementation: Whys, whens, and hows. Endocrine Reviews [Internet]. 2024 Apr 27;45(5):bnae009. Available from: https://pubmed.ncbi.nlm.nih.gov/38676447/
- Wang TJ, Pencina MJ, Booth SL, Jacques PF, Ingelsson E, Lanier K, et al. Vitamin D Deficiency and Risk of Cardiovascular Disease. Circulation [Internet]. 2008 Jan 29;117(4):503–11. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2726624/
- Norman PE, Powell JT. Vitamin D and cardiovascular disease. Circulation research [Internet]. 2014;114(2):379–93. Available from: https://www.ncbi.nlm.nih.gov/pubmed/24436433
- Shen H, Mei Y, Zhang K, Xu X. The Effect of Vitamin D Supplementation on Clinical Outcomes for Critically Ill Patients: A Systemic Review and Meta-Analysis of Randomized Clinical Trials. Frontiers in Nutrition. 2021 May 4;8.
- Aslam J, Sohailuddin M, Abbas SM, Muhammad, Saleem S, Arooj Mubeen, et al. The Schematic Assessment of Vitamin D Deficiency in Relation to Autoimmune Disorders and Its Implications in Internal Medicine. Cureus [Internet]. 2025 Apr 24; Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC12103644/
- Młynarska E, Lisińska W, Hossa K, Krupińska N, Jakubowska P, Rysz J, et al. Vitamin D and Chronic Disorders: A Review of Metabolic and Cardiovascular Diseases. Pharmaceuticals. 2025 Sep 29;18(10):1467.
- Atalan HK, Gucyetmez B. Serum Vitamin D Level at ICU Admission and Mortality. Turkish Journal of Anesthesia and Reanimation [Internet]. 2017 Aug 23 [cited 2025 May 20];45(4):193–6. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC5579211/?utm_source=chatgpt.com
- Raimondi S, Suppa M, Gandini S. Melanoma Epidemiology and Sun Exposure. Acta Dermato Venereologica. 2020;100(11):adv00136.
- Loney T, Paulo MS, Modenese A, Gobba F, Tenkate T, Whiteman DC, et al. Global evidence on occupational sun exposure and keratinocyte cancers: a systematic review. British Journal of Dermatology. 2020 Jun 30;184(2):208–18.
- Liu F, Grimsrud TK, Veierød MB, Robsahm TE, Ghiasvand R, Babigumira R, et al. Ultraviolet radiation and risk of cutaneous melanoma and squamous cell carcinoma in males and females in the Norwegian Offshore Petroleum Workers cohort. American Journal of Industrial Medicine [Internet]. 2021 Mar 8;64(6):496–510. Available from: https://www.duo.uio.no/bitstream/handle/10852/89674/ajim.23240.pdf?sequence=2
- A systematic review on UV exposure and the risk of keratinocyte carcinoma in people with darker skin colours | ARPANSA [Internet]. Arpansa.gov.au. 2022 [cited 2026 Jan 6]. Available from: https://www.arpansa.gov.au/systematic-review-uv-exposure-and-risk-keratinocyte-carcinoma-people-darker-skin-colours
- Arisi M, Zane C, Caravello S, Rovati C, Zanca A, Venturini M, et al. Sun Exposure and Melanoma, Certainties and Weaknesses of the Present Knowledge. Frontiers in Medicine [Internet]. 2018 Aug 30;5. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6126418/
- Lindqvist PG, Epstein E, Nielsen K, Landin-Olsson M, Ingvar C, Olsson H. Avoidance of sun exposure as a risk factor for major causes of death: a competing risk analysis of the Melanoma in Southern Sweden cohort. Journal of Internal Medicine. 2016 Mar 16;280(4):375–87.
- Weller RB. Sunlight: Time for a Rethink? The journal of investigative dermatology/Journal of investigative dermatology. 2024 Apr 1;
- Queirós CS, Freitas JP. Sun Exposure: Beyond the Risks. Dermatology Practical & Conceptual [Internet]. 2019 Oct 31;9(4):249–52. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6830553/
- Hoel DG, Berwick M, de Gruijl FR, Holick MF. The risks and benefits of sun exposure 2016. Dermato-Endocrinology [Internet]. 2016 Jan;8(1):e1248325. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5129901/
- Lindqvist PG, Epstein E, Landin-Olsson M, Måns Åkerlund, Olsson H. Women with fair phenotypes seem to confer a survival advantage in a low UV milieu. A nested matched case control study. PLoS ONE [Internet]. 2020 Jan 30 [cited 2025 Feb 4];15(1):e0228582–2. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC6992199/
- Ames BN, Grant WB, Willett WC. Does the High Prevalence of Vitamin D Deficiency in African Americans Contribute to Health Disparities? Nutrients [Internet]. 2021 Feb 3;13(2):499. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7913332/pdf/nutrients-13-00499.pdf
- Eggemoen ÅR, Knutsen KV, Dalen I, Jenum AK. Vitamin D status in recently arrived immigrants from Africa and Asia: a cross-sectional study from Norway of children, adolescents and adults. BMJ Open. 2013 Oct;3(10):e003293.
- Adebayo FA, Itkonen ST, Lilja E, Jääskeläinen T, Lundqvist A, Laatikainen T, et al. Prevalence and determinants of vitamin D deficiency and insufficiency among three immigrant groups in Finland: evidence from a population-based study using standardised 25-hydroxyvitamin D data. Public Health Nutrition [Internet]. 2020 May 1;23(7):1254–65. Available from: https://www.cambridge.org/core/journals/public-health-nutrition/article/prevalence-and-determinants-of-vitamin-d-deficiency-and-insufficiency-among-three-immigrant-groups-in-finland-evidence-from-a-populationbased-study-using-standardised-25hydroxyvitamin-d-data/B655B7514E0885292E80DAB19761B2C4
- Martin CA, Gowda U, Renzaho AMN. The prevalence of vitamin D deficiency among dark-skinned populations according to their stage of migration and region of birth: A meta-analysis. Nutrition. 2016 Jan;32(1):21–32.
- Hribar M, Igor Pravst, Pogačnik T, Katja Žmitek. Results of longitudinal Nutri-D study: factors influencing winter and summer vitamin D status in a Caucasian population. Frontiers in Nutrition [Internet]. 2023 Nov 15;10. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10684958/
- Ruiz-García A, Pallarés-Carratalá V, Turégano-Yedro M, Torres F, Sapena V, Martin-Gorgojo A, et al. Vitamin D Supplementation and Its Impact on Mortality and Cardiovascular Outcomes: Systematic Review and Meta-Analysis of 80 Randomized Clinical Trials. Nutrients [Internet]. 2023 Apr 7;15(8):1810. Available from: https://pubmed.ncbi.nlm.nih.gov/37111028/
- Zheng Y, Zhu J, Zhou M, Cui L, Yao W, Liu Y. Meta-Analysis of Long-Term Vitamin D Supplementation on Overall Mortality. Bencharit S, editor. PLoS ONE. 2013 Dec 3;8(12):e82109.
- Zhang X, Niu W. Meta-analysis of randomized controlled trials on vitamin D supplement and cancer incidence and mortality. Bioscience Reports. 2019 Nov;39(11).
- Gaksch M, Jorde R, Grimnes G, Joakimsen R, Schirmer H, Wilsgaard T, et al. Vitamin D and mortality: Individual participant data meta-analysis of standardized 25-hydroxyvitamin D in 26916 individuals from a European consortium. PLoS ONE [Internet]. 2017 Feb 16 [cited 2020 May 14];12(2). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5312926/
- Wu SE, Chen WL. Moderate Sun Exposure Is the Complementor in Insufficient Vitamin D Consumers. Frontiers in Nutrition. 2022 Mar 8;9(9).
- Raymond-Lezman JR, Riskin SI. Benefits and Risks of Sun Exposure to Maintain Adequate Vitamin D Levels. Cureus [Internet]. 2023 May 5;15(5). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10239563/
- Liu D, Fernandez BO, Hamilton A, Lang NN, Gallagher JMC, Newby DE, et al. UVA Irradiation of Human Skin Vasodilates Arterial Vasculature and Lowers Blood Pressure Independently of Nitric Oxide Synthase. Journal of Investigative Dermatology. 2014 Jul;134(7):1839–46.
- Queirós CS, Freitas JP. Sun Exposure: Beyond the Risks. Dermatology Practical & Conceptual [Internet]. 2019 Oct 31;9(4):249–52. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6830553/
- Mo Z, Scheben A, Steinberg J, Siepel A, Martienssen R. Circadian immunity, sunrise time and the seasonality of respiratory infections. 2021 Mar 31; Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC8020986/
- Cao M, He C, Gong M, Wu S, He J. The effects of vitamin D on all-cause mortality in different diseases: an evidence-map and umbrella review of 116 randomized controlled trials. Frontiers in Nutrition [Internet]. 2023 Jun 22;10. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10325578/
- Kift RC, Webb AR. Globally Estimated UVB Exposure Times Required to Maintain Sufficiency in Vitamin D Levels. Nutrients [Internet]. 2024 May 15;16(10):1489–9. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC11124381/
- Neale RE, Beedle V, Ebeling PR, Elliott T, Francis D, Girgis CM, et al. Balancing the risks and benefits of sun exposure: A revised position statement for Australian adults. Australian and New Zealand Journal of Public Health [Internet]. 2024 Feb 12;48(1):100117. Available from: https://www.sciencedirect.com/science/article/pii/S1326020023052949#:~:text=Results
- Sinclair C. Risks and benefits of sun exposure: Implications for public health practice based on the Australian experience. Progress in Biophysics and Molecular Biology. 2006 Sep;92(1):173–8.
- Webb A, Kazantzidis A, Kift R, Farrar M, Wilkinson J, Rhodes L. Colour Counts: Sunlight and Skin Type as Drivers of Vitamin D Deficiency at UK Latitudes. Nutrients. 2018 Apr 7;10(4):457.
- Weller RB, Mahrhofer M, Davis W, Gorman S. Risks and Benefits of UV Radiation. Current Problems in Dermatology [Internet]. 2021;55:329–38. Available from: https://pubmed.ncbi.nlm.nih.gov/34698040/
- Wacker M, Holick MF. Sunlight and Vitamin D. Dermato-Endocrinology. 2013 Jan 1;5(1):51–108.
- IARC moves sunbeds to highest cancer risk category [Internet]. Ecancer.org. ecancer; 2009. Available from: https://ecancer.org/en/news/658-iarc-moves-sunbeds-to-highest-cancer-risk-category
- Hoel D, de Gruijl F. Sun Exposure Public Health Directives. International Journal of Environmental Research and Public Health. 2018 Dec 10;15(12):2794.
- Porter E, Rafferty S, Dolan M, McMahon D, Sheikhi A, Field S, et al. The impact of a novel digital sun protection campaign on sun‐related attitudes and behaviours of healthcare workers: A prospective observational study. The impact of a novel digital sun protection campaign on sun‐related attitudes and behaviours of healthcare workers: A prospective observational study. 2023 Jun 8;
- Dessinioti C, Stratigos AJ. An Epidemiological Update on Indoor Tanning and the Risk of Skin Cancers. Current Oncology [Internet]. 2022 Nov 17;29(11):8886–903. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9689757/